Diagnostic accuracy of rapid diagnostic tests for the early detection of leptospirosis
Abstract
Background
Leptospirosis is often misdiagnosed with several other tropical febrile illnesses in Malaysia due to similarities in clinical manifestations. Although treatment regimens could be started based on clinical judgments, early diagnosis has become paramount as a guide to chemotherapeutic interventions. Confirmed laboratory diagnosis through MAT or PCR is time consuming and usually available only in reference laboratories and not practical in healthcare settings. Rapid and easy to perform diagnostic tests are widely used in these settings as the point of care diagnosis. The present study was undertaken to compare the diagnostic performance of two IgM based immunodiagnostic assay kits for acute leptospirosis.
Methods
A total of 50 serum samples were collected from patients clinically suspected for acute leptospirosis on admission in the Hospital Serdang, from June 2016 to June 2017. All the samples were subjected to MAT, lipL32 PCR and the two rapid tests (Leptocheck-WB and ImmuneMed Leptospira IgM Duo Rapid test).
Results
Out of the 50 clinically suspected patients sampled, 19 were confirmed positive for leptospirosis. Six (12%) were confirmed by MAT and 13 (26%) by PCR. Similarly, of the 50 clinically suspected cases, 17 (34%) showed positivity for Leptocheck-WB and 7 (14%) for ImmuneMed Leptospira IgM Duo Rapid test. The overall sensitivity and specificity was 47.37% and 80.65% for Leptocheck-WB, and 21.05% and 90.32% for ImmuneMed Leptospira IgM Duo Rapid test. In another set of previously confirmed MAT positive samples (1:400–1:3600) obtained from a reference laboratory, Leptocheck-WB showed higher sensitivity (90.72%) than ImmuneMed Leptospira IgM Duo Rapid test (40.21%), and comparable specificity for ImmuneMed Leptospira IgM Duo Rapid test (88.89%) and Leptocheck-WB (82.86%).
immunemed leptospira rapid
Conclusion
The sensitivity was higher for Leptocheck-WB and had a comparable specificity with ImmuneMed Leptospira IgM Duo Rapid test. Therefore, based on the present study, Leptocheck-WB is found to be a more sensitive rapid immunodiagnostic test for acute leptospirosis screening in hospital settings.
Introduction
The neglected tropical illness leptospirosis caused by the spirochete Leptospira, is now an alarming re-emerging zoonosis with a worldwide distribution. In Malaysia, leptospirosis is gazetted as a notifiable disease since December 2010. The number of cases according to the data from the Ministry of Health Malaysia (MOH) showed an increase from 3665 in 2012 to 5284 in 2016. Leptospirosis is a biphasic infection, the first phase (acute or septic phase) commences from 3 to 10 days of disease onset and the second phase (immune phase) ranges from 7 to 14 days .
During the acute phase, the bacteria can be found in the blood and then migrate and reside in the kidney where it continues to be shed in the urine. While in the second phase, a detectable number of antibodies develops and this stage coincides with the disappearance of the bacteria in the blood. Confirmatory laboratory diagnosis for leptospirosis involves testing for antigen (bacteria by culture or PCR of Leptospira pathogenic genes) in the first phase and antibodies in the second phase through the gold standard microscopic agglutination test (MAT).
Culture is not suitable for early diagnosis as Leptospira takes two weeks to four months to grow. On the other hand, PCR based detection, although gives a confirmatory diagnosis, it involves DNA extraction, technical expertise, expensive PCR machines and reagents, which limits the feasibility in many health care facilities. MAT is technically tedious and interpretations are very subjective and most importantly requires a greater panel of live leptospiral cultures to serve as antigens with the regular incorporation of new local and international serovars.
In Malaysia, MAT is available only at the National Leptospirosis Reference Centres such as the Institute for Medical Research located at capital Kuala Lumpur as well as the Zonal Public Health Laboratories. Considering all these shortcomings and challenges, a rapid test is highly desired and mostly preferred in hospitals in Malaysia, as it is a point of care test that can be performed in-house, and it is fast, technically simple and can be easily interpreted. It is pertinent to note that, there are several rapid tests commercially available which detect IgM antibodies produced against Leptospira antigens in the human serum. However, the sensitivity and the specificity vary for different kits in different geographical regions. To date, only two studies have evaluated commercially available rapid diagnostic kits for acute leptospirosis in Malaysia.
One of these studies, evaluated two commonly used rapid leptospirosis serological tests in Malaysia, Leptorapide(Linnodee, Northern Ireland) and VISITECT-LEPTO (Omega Diagnostics, Scotland, UK) reported limited diagnostic value in detecting acute leptospirosis as they showed lower sensitivities and specificities [11]. However, a more recent evaluation study on the IgM Duo Rapid test kit from Korea (immunochromatographic assay), showed a diagnostic sensitivity of 73% and specificity of 90%.
Nonetheless, a point of note regarding the aforementioned studies is that, both of them were performed on previously confirmed MAT/PCR positive samples rather than a prospective clinical evaluation of samples from patients in a hospital setting. As elsewhere, in Malaysia few serovars isolated locally are frequently observed among patients. Hence, it is also important to determine the diagnostic efficacy of any RDT against the locally isolated serovars as well.
The immune response to severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infection is initiated by innate immune activation followed by antigen-specific T and B cell responses. An important mechanism that protects against viral diseases is the presence of virus-neutralizing antibodies, which is similar for almost all viruses that cause acute illness followed by the elimination of pathogens.
Accordingly, all currently available antiviral vaccines are primarily intended to induce virus-neutralizing antibodies. Neutralizing antibodies generally block the binding of the virus to cell receptors.
In some cases, neutralizing antibodies can prevent the conformational changes necessary for virus fusion with the cell membrane or proteolytic cleavage. Neutralizing antibodies against SARS-CoV-2 are directed against the peak protein (S), which contains multiple antigenic epitopes in the receptor-binding domain (RBD) and non-RBD epitopes.
An important neutralization mechanism is to block the binding of RBD to angiotensin-converting enzyme 2 (ACE2), the virus’s cellular receptor. RBD is located at the tip of protein S. The receptor-binding motif (RBM) consists of approximately 70 aa within RBD and represents the actual amino acids that directly interact with ACE2.
Coronaviruses get their names from the typical spikes that are formed by the spike protein (S) that inserts into the lipid bilayer membrane of the virus. The receptor-binding domain (RBD) and its receptor-binding motif (RBM) allow interaction with the cell-surface receptor ACE2 that mediates entry of the virus into host cells.
This can be blocked by neutralizing antibodies. Therefore, most of the neutralizing epitopes are found on RBD / RBM. In addition to protein S, SARS-CoV-2 has two other viral surface proteins (not shown): envelope (E) and matrix (M).
Related Categories: Application rate, Biochemicals and reagents, Enzymes, Inhibitors and substrates, Isolation of proteins and nucleic acids
Quality level: 100
Form: lyophilized
Specific activity: ≥25 units / mg protein
Storage condition:
OK to freeze
Dried
Storage conditions: -20C
General description
Elastase is native to the porcine pancreas. Serine protease that catalyzes the hydrolysis of proteins and peptides (especially at bonds adjacent to neutral amino acid residues), including albumin, casein, denatured collagen, elastin, fibrin, and hemoglobin, and of various synthetic substrates containing aspartic acid, phenylalanine, or tyrosine. Inhibited by DFP, elastin, and α2-macroglobulin.
Elastase is native to the porcine pancreas. Catalyzes the hydrolysis of proteins and peptides (especially at bonds adjacent to neutral amino acid residues), including albumin, casein, denatured collagen, elastin, fibrin, and hemoglobin, and of various synthetic substrates containing aspartic acid, glutamic acid, phenylalanine, or tyrosine. Preferably it cleaves peptide bonds at the carbonyl end of amino acid residues with small hydrophobic side chains, such as glycine, valine, leucine, isoleucine, and particularly alanine. Inhibited by DFP, elastin, and α2-macroglobulin. It has an optimal pH of 7.8-8.5; pI = 9.5.
Packaging
1000, 250 u in plastic ampoule
Warning
Toxicity: Standard handling (A)
Definition of unit
One unit is defined as the amount of enzyme that will hydrolyze 1.0 mole of Suc-Ala-Ala-Pro-Abu-PNA (catalog # 324699) per minute at 25 ° C, pH 8.0.
Physical form
Lyophilized from 50 mM trehalose, 1 mM acetic acid.
Reconstitution
After reconstitution, elastase can be stored at 4 ° C at pH 6.0 for long-term use. If incubated at room temperature at or near its optimum pH, elastase rapidly autolyzes to a mixture of peptides. Stock solutions are stable for up to 2 months at 4 ° C, pH 6.0.
The product binds human IgG and not other human Ig. Immunoglobulins are composed of antigen-binding domains of two fragments (Fab) and one crystallizable fragment (Fc). The gene encoding the IgG gene cluster is found on human chromosome 14. Anti-human IgG antiserum (Fc specific) is produced in goat using purified human IgG, Fc fragment, as an immunogen. Affinity isolated antibody is obtained from goat anti-human IgG antiserum by immunospecific purification that removes essentially all goat serum proteins, including immunoglobulins, that do not specifically bind to the Fc fragment of human IgG.
Specificity
Specificity for the human IgG Fc fragment is determined by ELISA and immunoelectrophoresis (IEP). The antibody preparation is specific for human IgG, Fc fragment when tested against purified human IgA, IgG (Fc and Fab fragments), IgM, Bence Jones kappa, and Bence Jones lambda myeloma proteins. No reactivity is observed with the Fab fragment of human IgG, light chains, IgA or IgM. The affinity-purified anti-human IgG (Fc-specific) reagent offers the advantage of increased sensitivity for human IgG without cross-reactivity with other substances present on the cell membrane or surface.
The lack of cross-species cross-reactivity with mouse or rat serum proteins makes this product excellent for screening human monoclonal antibodies produced by hybridoma cells grown in vivo in mouse or rat ascites fluids. This product has the ability to detect all subclasses of human IgG in human biological fluids or tissues from normal or pathological situations such as cancer or autoimmune diseases. It is effective as a second antibody reagent in immunoassay procedures and can be used as a starting material for conjugates using enzymes or fluorescent dyes.
Immunogen
Anti-human IgG antiserum (Fc specific) is produced in goats using purified human IgG, Fc fragment, as an immunogen
Request
The anti-human IgG antibody (specific for Fc) produced in goats has been used:
in double capture ELISA to measure antiglobulin responses in the serum of transplant patients treated with monoclonal antibodies CD52 (CAMPATH-1G)
in the detection of IgG levels in patients with rheumatoid arthritis
in small bowel biopsies
in patients with acute myocardial infarction by immunoblotting
Physical form
The solution in 0.01 M phosphate-buffered saline, pH 7.4, containing 15 mM sodium azide
Storage and stability
For continuous use, store at 2-8 ° C for up to one month. For long-term storage, the solution can be frozen in working aliquots. Repeated freezing and thawing, or storing in “frost-free” freezers is not recommended. If slight cloudiness occurs after prolonged storage, rinse the solution by centrifugation before use.
Disclaimer
Unless otherwise stated in our catalog or other company documentation accompanying the product (s), our products are designed for research use only and are not to be used for any other purpose, including but not limited to commercial uses. unauthorized, in vitro diagnostic uses, ex vivo or in vivo therapeutic uses or any type of consumption or application to humans or animals.
Biochemical / Physiological Actions
The IgG antibody subtype is the most abundant of the serum immunoglobulins of the immune system. It is secreted by B cells and is found in blood and extracellular fluids and provides protection against infections caused by bacteria, fungi, and viruses. Maternal IgG is transferred to the fetus through the placenta, which is vital for the newborn’s immune defense against infection. Mutations in the Fc region of IgG are implicated in autoimmune diseases such as rheumatoid arthritis. Modified Fc proteins are of therapeutic importance for the treatment of autoimmune diseases.
Immunogen: Recombinant fragment containing amino acids 511-580 of human Glypican 3 (1G12); Full-length recombinant human GPC3 protein (GPC3 / 863)
Location: Cytoplasmic
Marker: Hepatocellular carcinoma marker
Specificity
Glypican-3 (GPC3) is an integral membrane protein that is mutated in Simpson-Golabi-Behmel syndrome (GBSS). SGBS is characterized by pre-and postnatal overgrowth and is an X-linked recessive condition. GPC3 can also be found in secreted form. Anti-GPC3 has been identified as a useful tumor marker for the diagnosis of hepatocellular carcinoma (HCC), hepatoblastoma, melanoma, testicular germ cell tumors, and Wilms tumor.
In HCC patients, GPC3 is overexpressed in neoplastic liver tissue and elevated in serum, but is undetectable in normal liver, benign liver, and serum from healthy donors. GPC3 expression is also found to be higher in HCC liver tissue than in cirrhotic liver or liver with focal lesions such as dysplastic nodules and areas of liver adenoma (HA) with malignant transformation. In the context of testicular germ cell tumors, GPC3 expression is up-regulated in certain histological subtypes, specifically yolk sac tumors and choriocarcinoma.
A high level of GPC3 expression has also been found in some types of embryonal tumors, such as Wilm’s tumor and hepatoblastoma, with low or undetectable expression in adjacent normal tissue. In thyroid cancer patients, GPC3 expression is dramatically improved in certain types of cancers: 100% in follicular carcinoma and 70% in papillary carcinoma. The expression of GPC3 in follicular carcinoma was significantly higher than that of follicular adenoma. In contrast, GPC 3 is not expressed in anaplastic carcinoma.
Isotype: IgG
Clonality: Monoclonal
Host: Mouse
Gene: GPC3
Purity: Purified Protein A or G
Innovator’s reward: Try on a species/app not listed above to receive a full credit towards a future purchase.
Applications / Dilutions
Dilutions
Flow cytometry 0.5 – 1 ug / million cells in 0.1 ml
Immunocytochemistry / Immunofluorescence 1-2 ug / ml
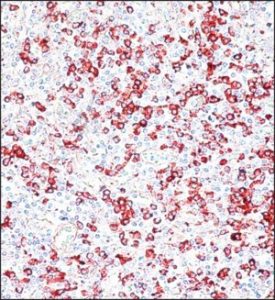
Immunohistochemistry
Immunohistochemistry-Paraffin 0.5 – 1.0 ug / ml
Immunofluorescence 0.5 – 1.0 ug / ml
Application notes
Immunohistochemistry (formalin-fixed): 1-2 ug/ml for 30 minutes at RT. Staining of formalin-fixed tissues requires heating tissue sections in 1 mM EDTA buffer, pH 7.5-8.5, for 45 min at 95 ° C followed by cooling at RT for 20 min.
The optimal dilution for a specific application must be determined.
Theoretical MW
67 kDa.
Disclaimer Note: The observed molecular weight of the protein may vary from the listed predicted molecular weight due to post-translational modifications, post-translation cleavages, relative charges, and other experimental factors.
Packaging, storage, and formulations
Storage: Store at 4C.
Buffer: 10 mM PBS with 0.05% BSA
Preservative: 0.05% sodium azide
Concentration: 0.2mg / ml
Purity: Purified Protein A or G
Alternative names for the Glypican 3 antibody (1G12 + GPC3 / 863)
DGSX
Glypican 3
glypican 3 proteoglycan
glypican-3
GPC3
GTR2-2
proteoglycan heparan sulfate
OCI-5 intestinal protein
MXR7
OCI5
OCI-5
glypican-3 secreted
SGB
SGBS
SGBS1SDYS
Limitations
This product is for research use only and is not approved for human use or clinical diagnosis. Primary Antibodies are guaranteed for 1 year from the date of receipt.
Anti-glycan antibodies are an abundant subpopulation of serum antibodies with critical functions in many immune processes. Changes in the levels of these antibodies can occur with the onset of disease, exposure to pathogens, or vaccination. As a result, there has been significant interest in exploiting anti-glycan antibodies as biomarkers for many diseases. The serum contains a mixture of anti-glycan antibodies that can recognize the same antigen, and competition for binding can potentially influence the detection of antibody subpopulations that are more relevant to disease processes.
The most abundant antibody isotypes in serum are IgG, IgM, and IgA, but little is known about how these different isotypes compete for the same glucan antigen. In this study, we developed a multiplexed glucan microarray assay and applied it to assess how different isotypes of anti-glucan antibodies (IgA, IgG, and IgM) compete for the imprinted glycan antigens. While IgG and IgA antibodies generally outperform IgM for peptide or protein antigens, we found that IgM outperformed IgG and IgA on many glucan antigens.
To illustrate the importance of this effect, we provide evidence that IgM competition may explain the unexpected observation that IgG of certain antigenic specificities appears to be preferentially transported from mothers to fetuses. We show that IgM in maternal serum competes with IgG resulting in lower than expected IgG signals. Since cord blood contains very low levels of IgM, competition only affects maternal IgG signals, making it appear that certain IgG antibodies are higher in cord blood than matched maternal blood. Taken together, the results highlight the importance of competition for studies involving anti-glycan antibodies.
Introduction
Human serum contains a wide variety of carbohydrate-binding antibodies that play a critical role in human health and provide a rich pool of potential biomarkers for many biomedical applications and diseases. For example, the detection of anti-glycan antibodies against blood group A and B antigens provides a simple and reliable strategy to predict which individuals are suitable for transfusion and transplantation. Anti-glycan antibodies are also crucial in other areas of immunology, such as tumor surveillance, autoimmunity, defense against pathogens, and response to vaccines.
These broader immune functions have stimulated interest in exploring the potential use of circulating anti-glycan antibodies as biomarkers for a wide variety of diseases. Detection of antiglycan antibodies in serum is typically carried out by immobilizing a carbohydrate of interest, capturing specific antibodies, and then measuring the amounts of bound antibodies.
This process is complicated by the fact that serum often contains a mixture of antibodies that recognize the same antigen, and certain antibodies within the mixture may be more relevant to immune protection or disease processes than others. Antibodies against a particular glycan can vary in terms of affinity, specificity, concentration, and/or isotype, but they can all compete to bind to the same antigen. As a result, the binding of one can influence the detection of the others, and it can be difficult to reliably measure a subpopulation of target antibodies of interest.
Results
Our approach to assessing competence involved the use of purified IgG, IgA, and IgM antibodies from pooled human serum. Each polyclonal antibody sample would be profiled on our glycan microarray individually and in the presence of other isotypes. In addition, changes in IgG and IgM anti-glycan antibody signals would be assessed in whole serum after the addition of IgG, IgA, and IgM. Although IgD and IgE are also present in serum at low concentrations and capable of competing, this study focused on the most abundant antibodies in serum.
Related categories: Cell culture, Cells, Hematopoietic stem cell culture, Human blood, and stem cell culture, Primary cell culture
Biological source: human umbilical cord blood
Packaging: 100,000 cells pack
Morphology: (parent)
Application (s): cell culture | mammal: suitable
Shipped: on dry ice
Storage temperature: −196 ° C
Request
CD34 is a glycosylated transmembrane protein and represents a well-known marker for primitive progenitor cells derived from blood and bone marrow, especially for hematopoietic and endothelial stem cells. Although the biological functions of CD34 are largely unknown, recent data suggest that CD34 is involved in maintaining progenitor cells in a phenotypically undifferentiated state.
PromoCell offers CD34 + progenitor cells from healthy donor umbilical cord blood. CD34 + progenitor cells contain two main cell subpopulations, hematopoietic and endothelial progenitor cells. Thus, CD34 + progenitor cells are suitable for a number of studies, e.g. Eg directed differentiation into more compromised blood cell types and endothelial lineages.
Quality
Rigid quality control tests are performed for each lot of CD34 + progenitor cells. They are routinely characterized by flow cytometry that analyzes viability, cell size, and the presence of significant markers, ie, CD34. Additionally, all cells have been tested for the absence of HIV-1, HIV-2, HBV, HCV, HTLV-1, HTLV-2, and microbial contaminants (fungi, bacteria, and mycoplasmas).
Warning
Although tests for HIV-1, HIV-2, HBV, HCV, HTLV-1, and HTLV-2 were negative, cells, like all products of human origin, should be handled as potentially infectious. No test procedure can completely guarantee the absence of infectious agents.
The protein encoded by this gene belongs to the angiotensin-converting enzyme family of dipeptidyl carboxypeptidases and has considerable homology to the human angiotensin 1 converting enzyme. This secreted protein catalyzes the cleavage of angiotensin I into angiotensin 1-9, and angiotensin II into the vasodilator angiotensin 1-7.
The organ- and cell-specific expression of this gene suggests that it may play a role in the regulation of cardiovascular and renal function, as well as fertility. In addition, the encoded protein is a functional receptor for the spike glycoprotein of the human coronavirus HCoV-NL63 and the human severe acute respiratory syndrome coronaviruses, SARS-CoV and SARS-CoV-2 (COVID-19 virus)
Coronaviruses are large, enveloped, positive-sense RNA viruses that are known to affect humans, birds, and mammals. These viruses have a genome length of 30 kb. The 5′-terminal of the viral genome encodes a polyprotein that upon cleavage yields several non-structural proteins that play important roles in viral transcription and replication. The 3′-terminal encodes 4 structural proteins, namely, Spike (S), Envelope (E), Membrane (M), and Nucleocapsid (N) that have an essential role in the synthesis of viral RNA and viral replication.
There are 6 known Coronaviruses that infect humans. Of these, two are known to cause severe diseases with high rates of mortality: Severe Acute Respiratory Syndrome Coronavirus (SARS-CoV) and Middle-East Respiratory Syndrome Coronavirus (MERS-CoV). Recently, a group of Chinese scientists discovered another strain of Coronavirus that caused a massive viral outbreak in China.
This virus is more deadly than SARS-CoV and MERS-CoV combined and is named SARS-CoV-2 (previously COVID-19). Since very little information available regarding the role of the COVID-19 proteins in viral pathogenesis and replication, not many treatment options are available. In addition to this, there are limited antibodies available in the market to detect these proteins.
BioVision is pleased to announce the launch of Coronavirus Antibodies, the first in the market. These antibodies specialize in detecting the Coronavirus disease 2019 nucleoprotein (SARS-CoV-2, COVID-19), SARS, and MERS. They have been tested using research techniques such as Western Blot, ELISA, Immunofluorescence, and Immunohistochemistry. These antibodies are available in both polyclonal and monoclonal formats and can readily be shipped worldwide.
Can these antibodies detect COVID-19/SARS-CoV-2?
Yes, some of our Coronavirus antibodies can detect COVID-19/SARS-CoV-2.
Nucleoprotein the positive strand of viral genome RNA into a helical ribbons leocapsid (RNP) and plays a fundamental role during virion assembly through its interactions with the viral genome and membrane protein M. It plays an important role in enhancing the efficiency of subgenomic viral RNA transcription as well as viral replication. Coronavirus nucleoproteins are phosphoproteins and are encoded near the 3′ end of the genome.
N possesses two RNA-binding domains: an N-terminal domain with adjacent S/R-rich motif and the C-terminal 209 amino acids. N protein is involved in coronavirus infection in many ways: the C-terminal domain (CTD) of N is important for binding the genomic RNA packaging signal leading to selective genome incorporation, the N3 domain interacts with the endodomain of M to form virions, and the serine–arginine repeat region of N (SR) interacts with the first ubiquitin-like domain of nsp3 in a critical early replication step.
Moreover, it has also been demonstrated that N can oligomerize through interactions in the CTD, bind viral RNA through the N-terminal domain, unwind double-stranded nucleic acid in the manner of an RNA chaperone, and pack in a helix through the N-terminal domain, though none of these other functions has yet been demonstrated to be important for infection.
Product Details
Description: Recombinant anti-SARS-CoV-2 Nucleoprotein Mouse ScFv is expressed from 293 cells (HEK293) with a human IgG1 Fc tag on C-terminal.
UniprotNo: P0DTC9
Alternative Names: Nucleocapsid protein, NC, protein N, N
Species Reactivity: Human Novel Coronavirus (SARS-CoV-2/ 2019-nCoV)
Immunogen Recombinant: Human Novel Coronavirus Nucleoprotein (N) (1-419aa) (CSB-EP3325GMY)
Immunogen: Species Human Novel Coronavirus (SARS-CoV-2/ 2019-nCoV)
Conjugate: Non-conjugated
Clonality: Monoclonal
Isotype Mouse scFv fusion with human IgG1 Fc
Clone No: 1A6
Purification Method: Affinity-chromatography
Concentration It differs from different batches. Please contact us to confirm it.
Buffer Preservative: 0.03% Proclin 300
Constituents: 50% Glycerol, 0.01M PBS, pH 7.4
Form: Liquid
Tested Applications: ELISA, WB, GICA
Storage: Upon receipt, store at -20°C or -80°C. Avoid repeated freeze.
Lead Time: Basically, we can dispatch the products out in 1-3 working days after receiving your orders. Delivery time maybe differs from different purchasing ways or locations, please kindly consult your local distributors for specific delivery time.